
Spinal Cord Injury
Directing Spinal Cord Plasticity: The Impact of Stretch Therapy on Functional Recovery After Spinal Cord Injury



Posted February 14, 2018
David S. K. Magnuson, Ph.D., University of Louisville

David S. K. Magnuson, Ph.D., University of Louisville

Anastasia Keller, Ph.D., University of Lousiville
A spinal cord injury (SCI) that results in partial paralysis below the point of injury is commonly accompanied by secondary complications such as joint contractures and spasticity. Currently, stretching remains the first line of therapy for patients with SCI in order to prevent contractures and maintain the extensibility of soft tissues. Despite its frequent application, there is little information on how stretching might influence neural circuitry in the spinal cord. With support from a fiscal year 2011 Investigator-Initiated Research Award from the Spinal Cord Injury Research Program (SCIRP), members of Dr. David S. K. Magnuson's laboratory at the University of Louisville are exploring the effects of stretching on locomotor function after SCI.
They previously found that a daily stretching protocol, similar to what is prescribed for humans with SCI, has a negative effect on locomotor recovery in rats with mild thoracic SCI. This dramatic, although temporary, disruption of locomotor functions prompted the present study - asking what the impact of stretch-based therapy is on animals with moderate and severe SCI, with special emphasis on the timing and intensity of stretching relative to the injury, and how this commonly prescribed therapy is having these effects.
This two-part study was carried out by a team of students and research technicians led by Dr. Anastasia Keller who was recently awarded her PhD for this work. The first part of this study investigated the effects of stretching on locomotor function at acute and chronic time points after moderately severe contusive SCI. In particular, the team sought to determine if there was a window of vulnerability within which an intense stretch-based therapy would disrupt locomotor recovery. Locomotor function was assessed in rats with SCI after the stretching protocol was initiated at 4 days (acute) or 10 weeks (chronic) post-injury. Locomotor deficits were evident in both acute and chronic animals, but the deficits in the chronic group were more pronounced. After cessation of the stretching protocol, locomotor function recovered to control levels within 2 weeks. These results suggest that spinal cord locomotor circuitry was especially vulnerable to the negative effects of stretching in chronic animals.
The second part of the study explored a dynamic range of motion stretching protocol as an alternative to the standard static stretching protocol seeking to determine if one or the other approach was less detrimental to locomotor function. Dynamic stretching is applied for a shorter total duration than static stretching, and yet the study found it also dramatically disrupted locomotor function. Though the physiological mechanism is not yet known, results suggest the combination of SCI and stretching induces a temporary disruption of locomotor circuitry.
Cumulative results from the studies raise (previously unforeseen) concerns regarding stretch-based therapy as standard of care following SCI, and may also implicate its potential to hinder recovery of locomotor function. Dr. Magnuson has started planning studies with colleagues at the Frazier Rehab Institute and Kentucky Spinal Cord Injury Research Center to study this phenomenon clinically with the goal of optimizing treatment for patients with SCI.
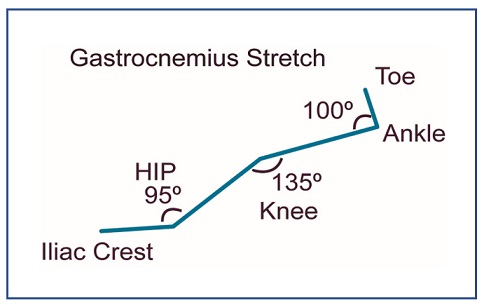
Gastrocnemius Stretch after Spinal Cord Injury
The stretching maneuvers utilized in these studies are modeled after those used commonly in the clinic. A full stretching protocol involves two, one-minute stretch-and-hold maneuvers for each major hindlimb muscle group, knee and ankle flexors and extensors plus hip adductors and hip abductors. Thus each muscle group experiences 2 minutes of stretching and the entire protocol takes approximately 30 minutes to administer.
The stretching maneuvers utilized in these studies are modeled after those used commonly in the clinic. A full stretching protocol involves two, one-minute stretch-and-hold maneuvers for each major hindlimb muscle group, knee and ankle flexors and extensors plus hip adductors and hip abductors. Thus each muscle group experiences 2 minutes of stretching and the entire protocol takes approximately 30 minutes to administer.
Link: