 An official website of the United States government
An official website of the United States government
 ) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
Peer Reviewed Medical
Comparative Effectiveness of Acupuncture for Chronic Pain and Comorbid Conditions
Posted June 24, 2022
Jun J. Mao, M.D., M.S.C.E., Memorial Sloan Kettering Cancer Center

Dr. Jun J. Mao
Chronic pain is a major health issue among Veterans, those in the military, and the American public. In the U.S. alone, the combined costs of health care for chronic pain patients and subsequent loss of productivity amount to $635 billion per year.1 For these patients the debilitating symptoms they exhibit can substantially affect their quality of life. The onset of the opioid crisis has further increased the challenge of reducing or eliminating chronic pain while mitigating risks of opioid misuse and abuse. Existing pain medications such as opioids, non-steroidal anti-inflammatories, and acetaminophen are not curative; instead, their constant use can lead to other ailments. Thus, comprehensive pain management techniques that do not incur risks of misuse or other harm are highly desirable. Acupuncture, a traditional medicine technique originating in Asiatic traditions, offers one such pain management treatment. In 2010, the Office of the Army Surgeon General published its Pain Management Task Force Final Report, in which they described acupuncture as a Tier I treatment modality, meaning that it was highly supported by scholarly literature for use as a treatment.2 Further, the Veterans Health Administration included acupuncture in its list of complementary and integrative health approaches covered by the Veterans' medical benefits package in 2017.3 Still, understanding when and for whom to use acupuncture therapies are key elements to its effective implementation as a pain management therapy. In Fiscal Year 2014, the Peer Reviewed Medical Research Program awarded funding for a Clinical Trial Award to the Memorial Sloan Kettering Cancer Center, led by Dr. Jun Mao, to address some of these unknowns.
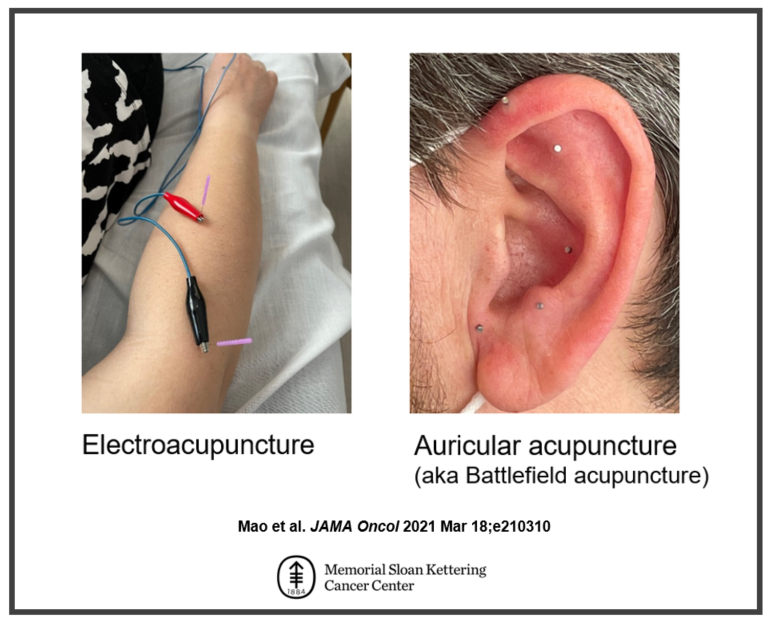
Figure 1: Electroacupuncture vs. Auricular acupuncture (aka Battlefield acupuncture). In electroacupuncture the needles are stimulated by a small electric current. It uses 4 points near the pain location and at least 4 other points across the body. Auricular acupuncture uses 10 semi-permanent needles on ear points (5 points per ear) and the needles are designed to stay in the ear for 3-4 days.
Dr. Mao conducted a randomized clinical trial in cancer survivors with chronic musculoskeletal pain comparing the effects of electro-acupuncture (a form of acupuncture where acupuncture needles are stimulated by a small electric current), battlefield acupuncture (a form of auricular acupuncture, or applied to ear), and a waitlist control group that received usual care after the other groups received treatment. In addition to determining which type of acupuncture is the most effective way to treat chronic musculoskeletal pain, Dr. Mao's group evaluated possible connections between the patient's acupuncture responses, the patient's expected outcomes from the therapy, and their genetic predisposition for responses to acupuncture. The study results were published in JAMA Oncology and showed that both electro-acupuncture and battlefield acupuncture decreased pain severity and improved mental and physical quality of life over time and at a higher rate when compared to usual care. Further, patients receiving these treatments reported decreased use of medications for pain management which was persistent even without additional use of acupuncture. Dr. Mao's team is also examining how a patient's expectation of the outcome affected their response to acupuncture treatment. Finally, they are evaluating how a patient's genetic makeup affected their response to acupuncture. Knowing who may respond to electro-acupuncture or battlefield acupuncture may allow patients and clinicians to choose the best treatment to maximize pain relief while reducing the chance of experiencing adverse effects.
The findings produced by Dr. Mao and his team add to the already substantial literature supporting acupuncture as an effective treatment modality for managing chronic pain. Additionally, their insights on patient expectations and genetic predispositions to electro-acupuncture will help patients and clinicians make the best decisions regarding a personalized treatment regimen for chronic pain. Dr. Mao now seeks to promote the adoption of battlefield acupuncture in settings where electro-acupuncture is not readily available. He also promotes systemic integration of both electro-acupuncture and battlefield acupuncture as part of a comprehensive pain management strategy to help patients at risk for opioid misuse due to their chronic pain.
Publications:
Mao JJ, Liou KT, Baser RE, et al. 2021. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors: The PEACE randomized clinical trial. JAMA Oncology 7(5):720:727.
Liou KT, Baser RE, Romero S, et al. 2020. Personalized electro-acupuncture versus auricular-acupuncture comparative effectiveness (PEACE): A protocol of a randomized controlled trial for chronic musculoskeletal pain in cancer survivors. Medicine 99(22):e20085
References:
1Care Committee on Advancing Pain Research (and Education), Institute of Medicine. 2010. Relieving pain in America: A blueprint for transforming prevention, care, education, and research. National Academies Press.
2https://dvcipm.usuhs.edu/tools-resources/pain-management-task-force.
3https://www.va.gov/WHOLEHEALTH/professional-resources/Acupuncture.
Links:
Last updated Tuesday, August 4, 2026