 An official website of the United States government
An official website of the United States government
 ) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
Prostate Cancer
Investigating Racial Differences in the Financial Impact of Prostate Cancer



Posted September 23, 2020
James Mohler, M.D., Roswell Park Comprehensive Cancer Center

The North Carolina–Louisiana Prostate Cancer Project (PCaP),1 led by Drs. James Mohler (Roswell Park) and Jeannette Bensen (University of North Carolina at Chapel Hill), was initially funded by the PCRP in FY02 and represents the largest population-based study of newly diagnosed prostate cancer in African American (AA) and Caucasian American (CA) men ever conducted, with 2,258 participants. The study published results in 2017 that demonstrated that racial differences in prostate cancer survival appear to originate more from a weak relationship of AA men with the American healthcare system, and poverty presents a significant obstacle to effective medical care for AA men compared to CA men. Thus while the Food and Drug Administration-approval of new treatments (e.g., immunotherapy, anti-androgens, radiopharmaceuticals, and chemotherapies) are extending the lives of patients with metastatic castration-resistant prostate cancer, the long-lasting side effects and large expense of these treatments places a significant financial burden and stress on prostate cancer patients and their families, and may contribute to disparate outcomes in AA prostate cancer patients.
In FY16, Dr. Mohler was awarded a Health Disparity Research Award to obtain 10-year follow-up data on the original group of prostate cancer patients from the PCaP and their caregivers. A critical goal of the project is to better understand the financial impact of prostate cancer treatment on patient survival and quality of life in both AA and CA men and to develop interventions to reduce the financial burdens and stress associated with a prostate cancer diagnosis. Dr. Mohler’s collaborators, including Dr. Ed Peters and his team at Louisiana State University Health Sciences Center School of Public Health are conducting surveys of PCaP participants and their caregivers through telephone, paper, and web-based questionnaires. Of the 1,331 living patients from the original group of PCaP patients, 561 (42% participation rate) have completed questionnaires and the data has been entered and quality checked. A very preliminary analysis compared financial distress in 194 patients by site (North Carolina, n= 76 versus Louisiana, n= 118) and by race (AA, n= 53 versus CA, n= 141), and the initial results showed slightly higher financial toxicity for AA respondents regardless of location (Figure 1).
Through this award, Dr. Mohler and his team are attempting to obtain electronic medical data using new methodology in both states. In Lousiana, the Surveillance, Epidemiology, and End Results (SEER) Program provides vital status and recurrence data that is enhanced through the PCORI-supported Louisiana REACHnet that accesses data from clinical practices, health care systems and insurance claims. In North Carolina, UNC’s Cancer Information and Population Health Resource has linkages to the North Carolina Central Cancer Registry and administrative and health insurance claims data from private payers, as well as, Medicare and Medicaid. The necessary agreements are almost in place to allow electronic collection of information on level of insurance coverage over the follow-up period, prostate cancer-specific treatments, medications, oncologic status, prostate-specific antigen (PSA) frequency and side-effects, which will be used to construct “OncoGraphs” on all participants. Some missing data will continue to be collected from living PCaP participants and their physicians in North Carolina and Louisiana. This rich dataset will provide valuable insight into the financial stress incurred by AA and CA prostate cancer patients and their families, and highlight socioeconomic disparities faced by those living with the disease. Furthermore, the dataset will provide a picture of the level of insurance coverage and level of care during the follow-up period for each participant, which may highlight further racial disparities during long term prostate cancer follow-up.
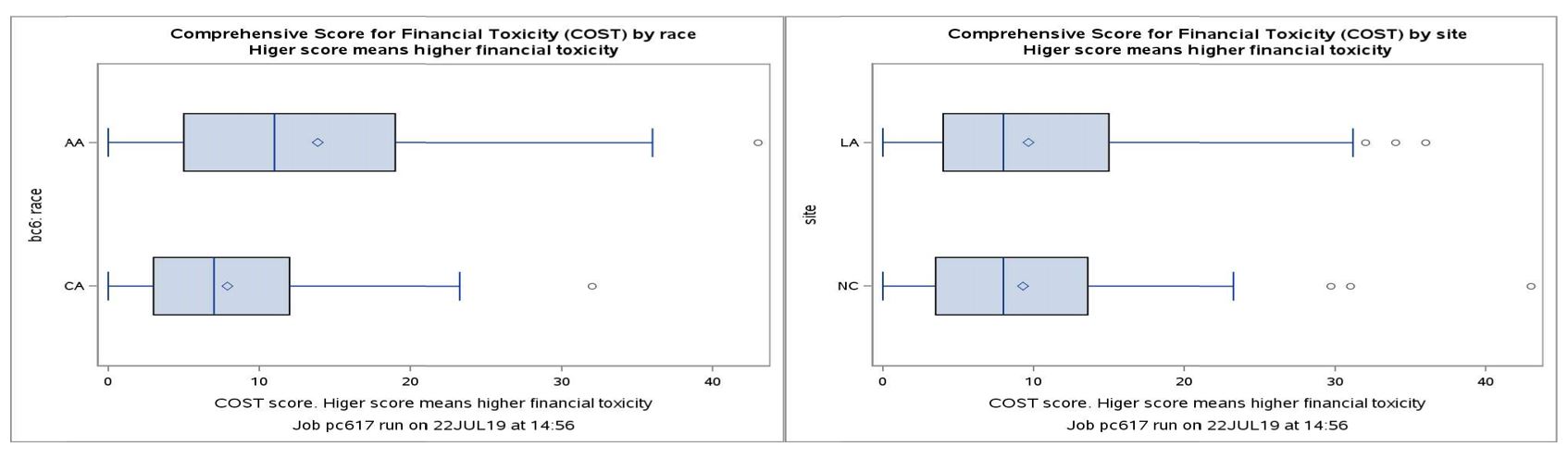 Figure 1. Comprehensive Score for Financial Toxicity (COST) by race and by state. The box is drawn from the first quartile (Q1) to the third quartile (Q3) with a vertical line going through the box at the median. The diamond marker inside the box indicates the mean value. Intra-quartile range (IQR) is the difference between the third and first quartile (IQR = Q3 – Q1). The whiskers that extend from each box indicate the range of values that are outside of the intra-quartile range (distance from the box is less than or equal to 1.5*IQR). Outliers (dot markers) are more extreme than -1.5/+1.5 IQR from the box.
Figure 1. Comprehensive Score for Financial Toxicity (COST) by race and by state. The box is drawn from the first quartile (Q1) to the third quartile (Q3) with a vertical line going through the box at the median. The diamond marker inside the box indicates the mean value. Intra-quartile range (IQR) is the difference between the third and first quartile (IQR = Q3 – Q1). The whiskers that extend from each box indicate the range of values that are outside of the intra-quartile range (distance from the box is less than or equal to 1.5*IQR). Outliers (dot markers) are more extreme than -1.5/+1.5 IQR from the box.
Reference:
North Carolina–Louisiana Prostate Cancer Project (PCaP): https://pcap.bioinf.unc.edu/
Link:
Public and Technical Abstracts: Racial Differences in Financial Impact of Prostate Cancer Treatment and Outcome
Last updated Friday, September 5, 2025