- Stromal Signaling Molecules as Potential Biomarkers of Metastatic Prostate Cancer
- The Prostate Cancer Clinical Trials Consortium (PCCTC): Multicenter Trials Made Easy
- Improved Radiation Therapy May Increase Prostate Cancer Survival
- Salmonella Mutant A1-R Cures Prostate Cancer in Metastatic Mouse Model
- Forging a Path from Trainee to Investigator
- The Role of SDF-1(Alpha)/CXCR4/MMP in PC Bone Metastasis
Stromal Signaling Molecules as Potential Biomarkers of Metastatic Prostate Cancer
Posted August 11, 2009
Neil A. Bhowmick, Ph.D., Vanderbilt University, Nashville, Tennessee
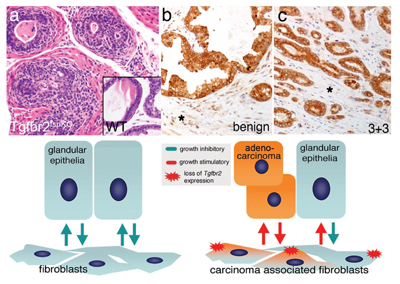
In the normal human prostate gland, the epithelial compartment (composed of basal, luminal, and rare neuroendocrine cells) forms ducts that are in close contact with an underlying stromal compartment (composed of smooth muscle, myofibroblasts, blood vessels, and occasional fibroblasts). Transforming Growth Factor beta (TGF-beta), is a signaling molecule that, while more highly expressed in the prostatic stromal compartment, plays an essential role in the normal differentiation of the prostatic epithelial cells. Dr. Neil Bhowmick, a recipient of Fiscal Year 2001 and 2003 Prostate Cancer Research Program New Investigator Awards, has proposed that the loss of TGF-beta signaling in stromal cells causes the overlying epithelial cells to become cancerous. To understand the role of TGF-beta in prostate gland development, Dr. Bhowmick developed a mouse model lacking the TGF-beta type II receptor (TGFBR2) in stromal cells. At 5 to 7 weeks of age, these mice developed spontaneous prostatic intraepithelial neoplasia (PIN) lesions, thought to be precursors to prostate cancer, showing that loss of TGFBR2 expression in the stroma can induce early signs of tumorigenesis. In another experiment, the role of TGF-beta in prostate cancer was further investigated by mixing human prostate cancer cells with mouse prostatic stromal cells and transplanting them into mice. The mice developed tumors, but tumors containing stroma derived from conditional TGFBR2 knockout mice were 5 times larger than those with stromal cells derived from normal (wild-type) mice, suggesting that loss of TGFBR2 expression in the stroma enhanced tumor progression. To relate these observations to human prostate cancer progression, TGFBR2 protein expression was assessed in a total of 140 benign and malignant prostate tumors from patients who had undergone radical prostatectomy using funding from other sources. Statistical analysis showed that the cancer samples were ten times less likely to show expression of stromal TGFBR2 than the benign prostate samples (p value < 0.0001).
As the recipient of a Fiscal Year 2008 Idea Development Award as well, Dr. Bhowmick plans to investigate the biological relevance of several signaling molecules produced by stromal cells whose expression has been shown to correlate with disease recurrence in prostate cancer patients. As recurrent disease following prostatectomy is indicative of metastatic cancer spread, and poor outcome for the estimated 27,000 U.S. men who will die from prostate cancer this year, these stromal-derived signaling molecules represent potential biomarkers for early detection and diagnosis of patients at risk of developing metastatic prostate cancer and potential therapeutic targets for more effective treatments.
(a) The loss of TGF-beta responsiveness in the prostate stroma leads to prostate cancer initiation in the stromal conditional knockout mouse model (Tgfbr2fspKO). (b) Benign human prostate tissue expresses TGF-beta type II receptor in both epithelial and stromal (asterisk) compartments. (c) Analogous to the conditional mouse knockout model, stromal loss of TGF-beta receptor type II expression is observed in human prostate cancer.
Publication:
Placencio VR, et al. 2008. Stromal transforming growth factor-beta signaling mediates prostatic response to androgen ablation by paracrine Wnt activity. Cancer Research 68:4709-4718.
Li X, et al. 2009. Urothelial transdifferentiation to prostate epithelia is mediated by paracrine TGF-beta signaling. Differentiation 77:95-102.
Li X, et al. 2008. Prostate tumor progression is mediated by a paracrine TGF-beta/Wnt3a signaling axis. Oncogene 27:7118-7130.
Link:
Public and Technical Abstracts: The Role of (beta)-Catenin in Androgen Receptor Signaling
The Prostate Cancer Clinical Trials Consortium (PCCTC): Multicenter Trials Made Easy
Posted July 7, 2009
In 2005, in response to gaps in clinical prostate cancer research identified by physician investigators and prostate cancer advocates, the U.S. Department of Defense (DOD) Prostate Cancer Research Program (PCRP) initiated the Prostate Cancer Clinical Trials Consortium (PCCTC) through the Clinical Consortium Award. The goal of this award was to accelerate and streamline the design, implementation, and completion of Phase I/II and Phase II clinical trials of novel agents and combination therapies that could prolong the lives of prostate cancer patients. In 2008, the PCRP expanded the PCCTC from 10 academic institutions to 13, and the PCCTC is now a major multi-institutional clinical research endeavor consisting of a nationwide network of leading institutions specializing in cutting-edge prostate cancer research with a single coordinating center located at Memorial Sloan-Kettering Cancer Center (MSKCC)*.
Capitalizing on their scientific expertise and unique institutional resources, Consortium members work together to design and execute Phase I/II and Phase II trials:
- more rapidly
- more efficiently
- with more precise readouts
- at a reduced cost
The Coordinating Center at MSKCC has implemented an organizational structure that allows for interactions between participating sites, regulatory agencies, trial sponsors, and internal and external advisory boards, and that ensures highly effective centralized management of PCCTC research activities. Harmonized scientific priorities, standard protocol and contract language, and centralized data management are just a few of the ways the Consortium evaluates needed therapies more efficiently.
The scientific framework of the program is the "clinical states model" of prostate cancer developed by the PCCTC, which divides the continuum of prostate cancer progression, for example, clinically localized versus metastatic disease, into milestones that guide clinical practice and research. Trials activated in the PCCTC span this clinical spectrum and include novel agents directed at unique targets and pathways like the investigational androgen receptor agonists Abiraterone and MDV3100. The Consortium also benefits from members' expertise in methodology and basic sciences. Biomarker development and target validation allow investigators to design trials with meaningful endpoints that distinguish promising approaches from ineffective ones. Leadership for the trials is equally distributed among Consortium members, reflecting the goal of accelerating therapeutic advances through multicenter collaboration and maximizing the diverse talents within each member institution.
In its first three years of formal existence, the PCCTC infrastructure facilitated the activation of over 60 Phase I or II clinical trials, 7 of which were first in human and 22 of which were first in prostate cancer. Approximately 30 different drugs, either in combination or alone, have been investigated, targeting five clinically defined stages of prostate cancer. The Consortium has recruited over 1,500 patients to these clinical trials and, of these, more than 10 percent of patients were recruited from disproportionately affected patient populations, demonstrating the PCRP and PCCTC's commitment to reducing prostate cancer health disparity among disproportionately affected populations.
The Consortium's successful acceleration and streamlining of the clinical trial process is a tribute to the collaborative nature and intellectual synergy of its members. PCCTC members have combined their scientific, clinical, and administrative expertise to ensure selection of promising drug candidates, design informative clinical endpoints, complete early-phase clinical trials as quickly as possible, and determine which drugs should advance to larger Phase III clinical trials. The PCCTC remains poised to make a significant impact on the lives of prostate cancer patients by keeping the pipeline primed with promising novel agents.
*MSKCC and other members of the PCCTC are also supported through the Prostate Cancer Foundation Therapeutic Clinical Investigation Consortium.
Publication:
Morris MJ, Basch EM, Wilding G, et al. 2009. Department of Defense Prostate Cancer Clinical Trials Consortium: A New Instrument for Prostate Cancer Clinical Research. Clinical Genitourinary Cancer 7(1):51-57.
Improved Radiation Therapy May Increase Prostate Cancer Survival
Posted June 24, 2009
Lei Xing, Ph.D., Stanford University School of Medicine, Stanford, California
One in every six men is diagnosed with prostate cancer during his lifetime, making it the second leading cause of cancer-related mortality among American males. Intensity modulated radiation therapy (IMRT) is replacing conventional three-dimensional conformal therapy to become the standard for external beam radiotherapy treatment for prostate cancer. Clinical studies have revealed that there is a strong correlation between high radiation dose and improved local control of disease. However, increased doses of radiation can lead to radiation toxicity and increased risk of developing gastrointestinal and genitourinary complications. Dr. Lei Xing, recipient of a Department of Defense Prostate Cancer Research Program (PCRP) Fiscal Year 2004 Idea Development Award, has developed an innovative algorithm to improve computer control of IMRT by employing a novel inverse planning scheme incorporating nonuniform importance factors. The advantage of this technique for treating patients is that radiation dose to the prostate tumor can be escalated by approximately 10%, without compromising the doses to sensitive structures surrounding the prostate gland such as the bladder, bowel, or rectum. Additionally, IMRT inverse planning for localized prostate cancer is faster, more robust, and reduces the treatment beam-on time delivery by at least 60%. Using this new software coupled with enhanced onboard cone-beam computed tomography (CBCT)-based patient localization and a real-time MV/kV image guidance technique developed by Dr. XingÂ’s group, it is estimated that the 5-year disease-free survival rate could increase from the current 48% to 75% for locally advanced prostate cancer patients through effective dose escalation. Dr. Xing is optimistic that this new technique could become standard clinical practice within 3 years, pending licensing, testing, and FDA approval. In addition to his scientific contributions, Dr. Xing has proven to be an outstanding mentor to two young scientists funded under a FY05 PCRP Postdoctoral Traineeship Award, who have obtained faculty positions at major university medical centers.
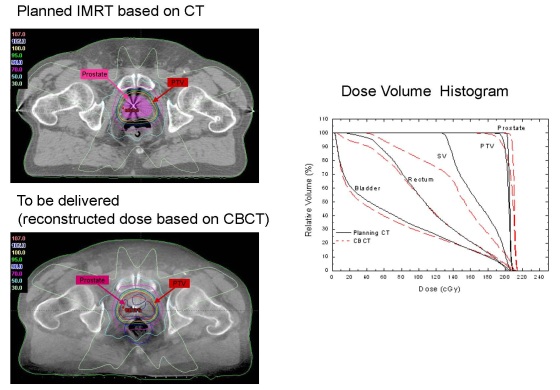
Comparison of computed tomography (CT) versus cone-beam computed tomography (CBCT) for IMRT Dose Verification. Dose distribution through a transverse slice of a patient for IMRT planning as determined by CT scan (top, left) and CBCT scan (bottom, left) showing the prostate gland in pink and the planning target volume (PTV) highlighted by the red circle. A dose volume histogram (DVH) of the prostate, seminal vesicles (SV), rectum, and bladder as well as the PTV based on CT and CBCT images (right).
Publications:
Zhu L, Lee L, Ma Y, Ye Y, Mazzeo R, Xing L. 2008. Using total-variation regularization for intensity modulated radiation therapy inverse planning with field-specific numbers of segments. Phys Med Biol 53(23):6653-72. (Epub 2008 Nov 7)
Yang Y, Schreibmann E, Li T, Wang C, Xing L. 2007. Evaluation of on-board kV cone beam CT (CBCT)-based dose calculation. Phys Med Biol 52:685-705.
Link:
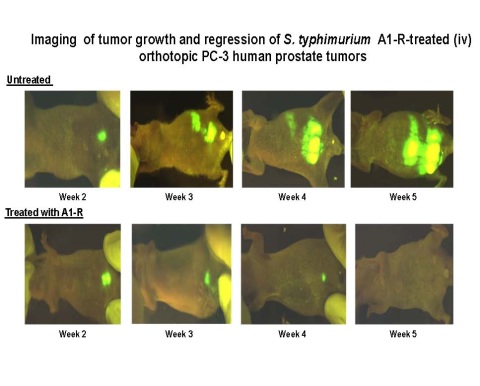
Salmonella Mutant A1-R Cures Prostate Cancer in Metastatic Mouse Model
Posted April 23, 2009
Ming Zhao, M.D., Ph.D., AntiCancer Incorporated
Dr. Ming Zhao, recipient of a Fiscal Year 2005 Idea Development Award, has developed a strain of Salmonella typhimurium (S. typhimurium) that can target and kill metastatic prostate cancer cells in mice without the addition of chemotherapy. It has long been known that anaerobic bacteria, such as S. typhimurium, can grow selectively in hypoxic and necrotic regions of tumors. Dr. Zhao's S. typhimurium strain, termed A1-R, is a leu-arg auxotroph which helps restrict growth in normal tissues and favors growth in necrotic areas of tumors. A1-R was also engineered to express green fluorescent protein (GFP) to visualize bacteria growth in live mice. To test the antitumor efficacy of A1-R, mice with implanted orthotopic PC-3 human prostate tumors received weekly intravenous injections of the A1-R bacteria. The biodistribution ratio of A1-R in tumor to normal tissue was approximately 106, indicating a very high degree of tumor targeting by A1-R. Tumor size in the treated group was approximately 75% smaller than the untreated group by day 30 after implantation (n = 10, P =0.04). Metastasis occurred by day 21 after tumor implantation in the untreated mice, and by day 30 the metastases had spread to other organs. All of the untreated mice died within six weeks of tumor implantation. In contrast, metastatic tumors in the mice treated weekly with A1-R grew slowly or disappeared completely. Seventy percent of these mice were alive on day 40, when the last untreated mouse died. A1-R treatment resulted in a doubling of the 50% survival time compared to untreated mice. In addition, 40% of the A1-R treated mice remained alive six months after tumor implantation and were essentially cured of prostate cancer. Tumors did not return after treatment stopped. Also, no toxic effects were detected in non-tumor bearing mice treated with weekly injections of A1-R.
To further understand how Salmonella bacteria preferentially target tumor tissue, Dr. Zhao has obtained additional funding resources to screen Salmonella promoter libraries. Her ultimate goal is to develop the expression of therapeutics in bacteria under the regulation of promoters that are preferentially expressed in tumor tissue to improve the targeting of drug delivery. This work paves the way toward the development of a novel form of targeted therapy with the potential for impacting not just prostate cancer, but other cancers as well.
Publications:
Zhao M, Geller J, Ma H, et al. 2007. Monotherapy with a tumor-targeting mutant of Salmonella typhimurium cures orthotopic metastatic mouse models of human prostate cancer. Proceedings of the National Academy of Sciences of the United States of America 104:10170-10174.
Arrach N, Zhao M, Porwollik S, et al. 2008. Salmonella promoters preferentially activated inside tumors. Cancer Research 68:4827-4832.
Link:
Public and Technical Abstracts: Targeting Prostate Cancer with Tumorocidal Bacteria

Forging a Path from Trainee to Investigator
Posted April 9, 2009
Arun Sreekumar, Ph.D., University of Michigan, Ann Arbor, Michigan
Photo used with permission of D.K. Bhaskar.
The Prostate Cancer Research Program (PCRP) aims to support research that will one day lead to the eradication of prostate cancer. With this overarching goal in mind, the PCRP understands that success relies heavily on the training of new investigators in the field of prostate cancer. One notable young scientist, Dr. Arun Sreekumar, is forging a path to help realize this vision.
Dr. Sreekumar of the University of Michigan received a Fiscal Year 2002 PCRP Postdoctoral Traineeship Award to study prostate cancer profiles using protein microarrays, with the goal of discovering novel biomarkers and developing new, noninvasive methods to detect prostate cancer. Through this funding, he created a microarray specific to prostate cancer proteins and used it to examine the sera from prostate cancer subjects and controls. He then was able to determine an "epitomic profile" of prostate cancer by identifying autoantibodies generated by the body against prostate cancer proteins. Overall, Dr. Sreekumar identified multiple prostate cancer biomarkers and demonstrated that they were detectable with high sensitivity and specificity in urine and serum via high throughput western blotting.
These findings may lead to a more robust method for the accurate and early detection of prostate cancer utilizing multiple prostate cancer biomarkers including alpha-methylacyl-CoA Racemase (AMACR). Dr. Sreekumar's research led to four publications and two patents that will advance prostate cancer diagnostics and may enable caregivers the ability to detect prostate cancer with greater accuracy and specificity.
Recently, Dr. Sreekumar received his first R01 award from the National Cancer Institute to research cellular metabolism during prostate cancer progression. This achievement marks Dr. Sreekumar's successful transition, with the support of the PCRP, from trainee to independent investigator, and underscores the PCRP's emphasis on the training of young investigators in prostate cancer research to expand scientific knowledge and find new therapies to conquer this disease. Dr Sreekumar's latest success involves the potential identification of a new prostate cancer biomarker, sarcosine, by examining the metabolomic profiles of prostate cancer patients.
Publications:
Wang X, Yu J, Sreekumar A, Varambally S, Shen R, Giacherio D, Mehra R, Montie JE, Pienta KJ, Sanda MG, Kantoff PW, Rubin MA, Wei JT, Ghosh D, Chinnaiyan AM. 2005. Autoantibody signatures in prostate cancer. N Engl J Med. 353(12):1224-1235.
Bradley SV, Oravecz-Wilson KI, Bougeard G, Mizukami I, Li L, Munaco AJ, Sreekumar A, Corradetti MN, Chinnaiyan AM, Sanda MG, Ross TS. 2005. Serum antibodies to huntingtin interacting protein-1: A new blood test for prostate cancer. Cancer Res 65(10):4126-4133.
Sreekumar A, Laxman B, Rhodes DR, Bhagavathula S, Harwood J, Giacherio D, Ghosh D, Sanda MG, Rubin MA, Chinnaiyan AM. Humoral immune response to alpha-methylacyl-CoA racemase and prostate cancer. 2004. J Natl Cancer Inst 96(11):834-843.
Yan F, Sreekumar A, Laxman B, Chinnaiyan AM, Lubman DM, Barder TJ. 2003. Protein microarrays using liquid phase fractionation of cell lysates. Proteomics 3(7):1228-1235.
Link:
Public and Technical Abstracts: Profiling Prostate Cancer Using Protein Microarrays

The Role of SDF-1(Alpha)/CXCR4/MMP in PC Bone Metastasis
Posted March 13, 2009
Sreenivasa R. Chinni, Ph.D., Wayne State University School of Medicine and the Barbara Ann Karmanos Cancer Institute, Detroit, Michigan
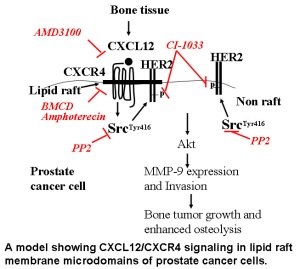
Prostate cancer metastasis is the primary cause of mortality in patients. Dr. Chinni, of Wayne State University, received a fiscal year 2002 (FY02) PCRP New Investigator Award to study the role of chemoattractive mechanisms in prostate cancer bone metastasis. Chemokines and their receptors play a role in tumor cell migration and homing of metastatic cells to target tissues. Prior work in this area has suggested that the interaction of chemokine ligand stromal cell-derived factor-1 alpha (SDF-1a, also known as CXCL12) to its receptor, CXCR4, plays a crucial role in site-specific metastasis of several cancers. On this basis, Dr. Chinni proposed to investigate the hypothesis that CXCR4 and SDF-1a play a role in prostate cancer bone metastasis as well. Using a variety of techniques, Dr. Chinni and colleagues were able to detect expression of both CXCR4 and SDF-1a in prostate cancer cells and human fetal bone stromal cells. They found that migration of PC-3 prostate cancer cells in bone co-cultures was dependent on SDF-1a/CXCR4 signaling and SDF-1a activated Akt kinase via the PI3-kinase pathway. Additionally, they were able to show that SDF-1a induced expression of the protease, matrix metallopeptidase 9 (MMP-9), in prostate cancer cells. MMPs promote tumor progression and metastasis by degradation of the extracellular matrix and, in addition, promote angiogenesis, a process required for tumor growth. Western blot analysis of PC-3 and LNCaP prostate cancer cells showed that CXCR4 protein was localized to lipid rafts. Lipid rafts are microdomains that modulate oncogenic signal transduction by maintaining steady state levels of growth factor receptors. Gene expression profiles revealed that several members of the protease and chemokine families were upregulated in CXCR4-overexpressing PC-3 cells. These data suggest that chemoattractive mechanisms may be involved in migration of prostate cancer cells toward bone tissue, and that cell signaling induced by binding of the chemokine to its receptor leads to the activation of multiple signaling pathways, including subsequent release of MMPs into the local environment. These findings may provide a link between chemoattractive mechanisms, growth of tumor cells in bone, and tumor-enhanced bone matrix turnover. Dr. Chinni has also received a FY08 PCRP Idea Development Award to study upstream regulators of CXCR4 expression including androgens and ERG family transcription factors (TMPRSS2-ERG translocations) and downstream effects following CXCR4 activation in prostate cancer models.
Publications:
Chinni SR, Sivalogan S, Dong Z, et al. 2006. CXCL12/CXCR4 signaling activates Akt-1 and MMP-9 expression in prostate cancer cells: the role of bone microenvironment-associated CXCL12. The Prostate 66(1):32-48.
Chinni SR, Dong Z, Hamilton Y, et al. 2008. CXCL12/CXCR4 trans-activates HER2 in lipid rafts of PC cells and promotes in vivo intra-osseous tumor growth. Molecular Cancer Research 6(3):446-457.
Link:
Public and Technical Abstracts: The Role of SDF-1(Alpha)/CXCR4/MMP in PC Bone Metastasis