 An official website of the United States government
An official website of the United States government
 ) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
Lung Cancer



Posted November 1, 2023
Scott Antonia, M.D., Ph.D., and Chuan-Yuan Li, Ph.D., Duke University
Non-small cell lung cancer (NSCLC) will account for approximately 80% to 85% of the estimated 238,340 new lung cancer diagnoses in the United States in 2023.1 NSCLC and other cancers can evade the activity of cytotoxic T cells, a cell-killing immune cell, by displaying immune checkpoint proteins. These proteins signal to the immune system that cancer cells are normal and healthy, preventing T cell activation. Immune checkpoint inhibitors (ICIs) are antibodies used to disrupt this signaling, permitting T cells to recognize cancer cells as abnormal and destroy them. Since only 20% of patients respond to single ICI immunotherapy,2 most patients with NSCLC receive combination treatment with multiple ICIs.
 Dr. Scott J Antonia
Dr. Scott J Antonia
(Photo provided)
 Dr. Chuan-Yuan Li
Dr. Chuan-Yuan Li
(Photo provided)
From a fiscal year 2020 Lung Cancer Research Program Clinical Translational Research Partnership Award, Dr. Scott Antonia and Dr. Chuan-Yuan Li are conducting a pilot clinical trial3 to evaluate the safety and effectiveness of a novel immunotherapy regimen for the treatment of NSCLC. This regimen combines ICIs with an antibody against a protein called PCSK9, which when secreted by tumor cells, reduces the concentration of a protein called MHC-I on the cell surface. MHC-I is required for T cells to recognize and kill tumor cells, so in reduced concentration, T cell engagement and antitumor immune activity is inhibited, even after immune checkpoints are blocked by ICIs. The team hypothesizes anti-PCSK9 antibodies will restore the concentration of MHC-I on tumor cells by blocking the activity of PCSK9. They anticipate the novel treatment regimen will initiate twofold antitumor activity: (1) ICIs will prevent tumor cells from disguising themselves as healthy and evading T cells, and (2) anti-PCSK9 antibodies will enhance T cell binding to tumor cells, enabling cell killing activity.
The pilot clinical trial compares two treatment groups. One group of participants is receiving standard-of-care therapy comprised of two ICIs – nivolumab and ipilimumab – that bind to different immune checkpoint proteins. The other group is receiving this therapeutic combination in addition to an anti-PCSK9 antibody called evolocumab. The research team collects tumor biopsy samples before and during treatment to determine whether adding evolocumab to the standard treatment regimen increases MHC-I concentration and infiltration of immune cells into tumor tissue. They also monitor disease progression of each participant throughout the trial using the standard RECIST criteria (response evaluation criteria in solid tumors), which are applied to radiographic images of tumors over time to evaluate changes in size and appearance. The team will use tumor biopsy and radiographic data to compare the effects of adding evolocumab to the established ICI treatment regimen. As of July 2023, 11 patients are enrolled in the clinical trial, and data analyses are ongoing.
In previous studies, the team identified another protein called, ATM, they believe may further enhance the activity of the combined treatment regimen, as inhibition of ATM demonstrated increased expression of MHC-I on the cell surface. In follow-up studies using mouse models and three-dimensional human tumor model systems, the team intends to determine whether adding an ATM inhibitor to the treatment regimen synergizes with evolocumab to further enhance ICI immunotherapy. Since the FDA already evaluated the individual components of these combination therapies, they could be implemented into clinical practice sooner than newly developed drugs. If successful, this novel regimen may expand the use of ICIs to previously excluded patients with low MHC-I, improving immunotherapy for NSCLC.
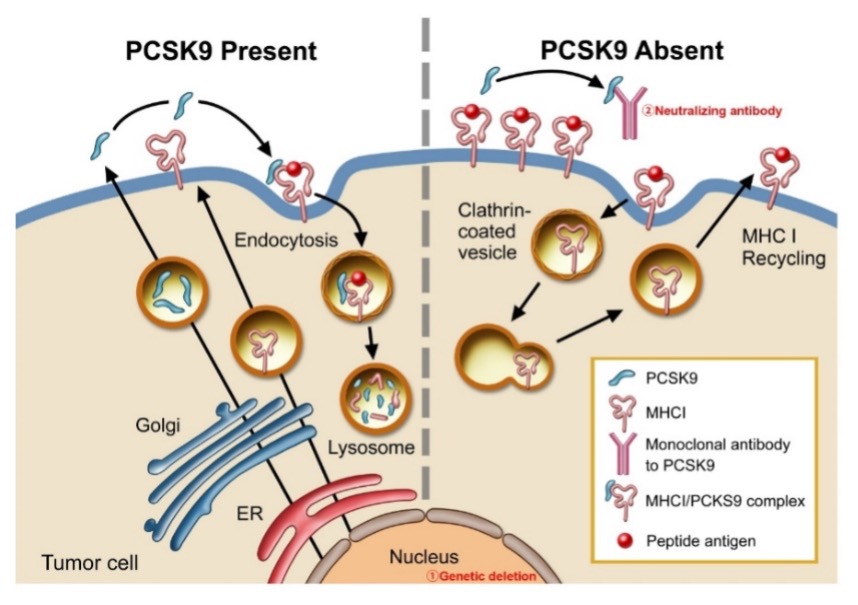 Fig. 1. A schematic diagram illustrating PCSK9-mediated degradation of MHC I in the lysosome. In the presence of PCSK9, MHC I was transported into the lysosome and degraded (left panel). In the absence of PCSK9, either because of antibody-mediated neutralization or genetic deletion, MHC I levels on the tumor cell surface remained high and was thus able to present tumor-specific peptide antigens more efficiently to T cells (right panel). Liu et al, Nature, 2020, PMID:33177715. (Figure provided)
Fig. 1. A schematic diagram illustrating PCSK9-mediated degradation of MHC I in the lysosome. In the presence of PCSK9, MHC I was transported into the lysosome and degraded (left panel). In the absence of PCSK9, either because of antibody-mediated neutralization or genetic deletion, MHC I levels on the tumor cell surface remained high and was thus able to present tumor-specific peptide antigens more efficiently to T cells (right panel). Liu et al, Nature, 2020, PMID:33177715. (Figure provided)
References:
1Key Statistics for Lung Cancer. American Cancer Society. https://www.cancer.org/cancer/types/lung-cancer/about/key-statistics.html
2Ribas A and Wolchok JD. 2018. Cancer immunotherapy using checkpoint blockade. Science 359(6382):1350-1355. https://doi.org/10.1126/science.aar4060
3A Randomized Pilot Study of Evolocumab Plus Nivolumab/Ipilimumab in Treatment-Naïve Patients With Metastatic NSCLC (TOP2101). ClinicalTrials.gov. https://clinicaltrials.gov/study/NCT05144529
Last updated Monday, June 29, 2026