



Posted May 12, 2015
Robert F. Buckman, Jr., M.D., Operative Experience, Inc., North East, Maryland
 Combat Casualty Care demands that a variety of trauma skills be practiced by first responders, medics, nurses, physicians and other healthcare workers. There is a need for rapid and effective training of deploying surgeons. Current training programs in trauma care often do not provide "hands-on" experiences for both naïve physicians as well as experienced surgeons, who may be experiencing skill decay over time. Operative Experience, Inc. (OEI) meets this need with a series of novel short-term courses that combine physical models with multimedia training modules in war surgery. Led by Dr. Robert F. Buckman, Jr., this project has produced a series of physical models, with high anatomic fidelity, that are able to provide realistic hands-on training experiences for physicians.
Combat Casualty Care demands that a variety of trauma skills be practiced by first responders, medics, nurses, physicians and other healthcare workers. There is a need for rapid and effective training of deploying surgeons. Current training programs in trauma care often do not provide "hands-on" experiences for both naïve physicians as well as experienced surgeons, who may be experiencing skill decay over time. Operative Experience, Inc. (OEI) meets this need with a series of novel short-term courses that combine physical models with multimedia training modules in war surgery. Led by Dr. Robert F. Buckman, Jr., this project has produced a series of physical models, with high anatomic fidelity, that are able to provide realistic hands-on training experiences for physicians.
Since 2009, the progress of OEI has been overseen by the Telemedicine and Advanced Technology Research Center (TATRC) as well as the Medical Simulation and Information Sciences Joint Program Committee. - 1 (JPC-1). The project began with funding from the Small Business Innovation Research (SBIR) program and subsequently received enhancement funding from JPC-1 and is currently being managed by the Congressionally Directed Medical Research Program office. OEI has created simulation-based training for more than 20 critical trauma skills for war surgery. Each training system includes physical models and multimedia instructional guide.
OEI's initial SBIR focused on lower extremity trauma care. Phase I culminated in a simulator for training in four-compartment fasciotomy of the lower leg. Phase II extended this research, resulting in simulation-based training in the fasciotomy of the thigh, below-knee and above-knee amputations, external fixation of the femur and extensile exposure of the femoral vessels as well as exposure and control of the femoral artery at the groin. Subsequent SBIR funding through TATRC has resulted in a craniectomy simulator for relief of a subdural hematoma; hemorrhage control training including tourniquet, junctional tourniquet, and wound packing; external fixation of the femur; shunting of the femoral artery; proximal control of the femoral artery at the groin; canthotomy; emergency thoracotomy; and emergency bi-lateral thoracotomy. The thoracotomy model includes an operable beating heart. Surgical models have artificial skin with realistic properties that can be incised and sutured, subcutaneous tissue, embedded periosteum-covered bones, articulated joints, major muscle groups, integrated dissection planes, fascia, and branching hollow blood vessels. Pre-hospital combat casualty care training has been facilitated by the development of a set of five soldier-form simulators with wound patterns that reflect an Improvised Explosive Device detonation followed by an ambush. Simulated wounds include burn, blast, high velocity gunshot wounds, and traumatic amputations. All of these models have been commercialized. Customers include U.S. Marine Corps, U.S. Department of State, and Uniformed Services University of the Health Sciences.
OEI seeks to provide standardized, simulation-based training systems to provide deploying combat surgeons with surgical practice and testing. They recently received additional Phase II funding to develop an abdominal trauma training system. OEI is working toward a library of comprehensive training that prepares surgeons and medics for life-saving combat casualty care skills.
(Photos below courtesy of Operative Experience, Inc.)
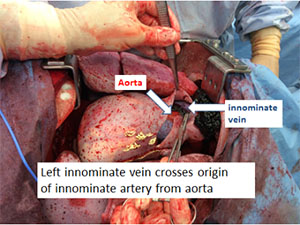
Figure 1. Anatomic model with exposure of innominate artery through bilateral trans-sternal thoracotomy. Anatomical model has beating heart and pulsatile blood flow.
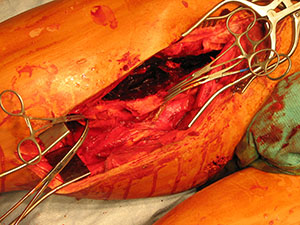
Figure 2. Exploration of high velocity gunshot wound to thigh on OEI simulator using standard surgical instruments.

Figure 3. Soldier-form manikin with gunshot wound entering beneath the left eye and exiting on the right side of the neck. Model includes a jaw fracture and disruption to tongue.