



Posted February 6, 2014
Brad M. Isaacson, PhD; The Henry M. Jackson Foundation for the Advancement of Military Medicine & The Center for Rehabilitation Sciences Research, Uniformed Services University of Health Sciences
Paul F. Pasquina, MD; Benjamin K. Potter, MD; Roy D. Bloebaum, PhD; Thomas M. Swanson, BA; Dustin L. Williams, PhD; Richard T. Epperson; Brooke Kawaguchi
 Heterotopic ossification (HO) typically manifests in the residual limb and/or the joint space following traumatic orthopedic and/or neurological injury. Given the intense nature of blast injuries, which require rapid tourniquet use, debridement and surgical intervention, HO has been reported to occur in approximately 63%-65% of service members with limb loss or major extremity injuries during Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF). Reports of recent OIF/OEF combat-related amputees with known HO have indicated that approximately 20-40% of affected patients required surgery to excise bony masses. HO may cause skin ulcerations, chronic pain, and delay rehabilitation regimens, as ectopic bone resection often requires modifications to the prosthetic limb.
Heterotopic ossification (HO) typically manifests in the residual limb and/or the joint space following traumatic orthopedic and/or neurological injury. Given the intense nature of blast injuries, which require rapid tourniquet use, debridement and surgical intervention, HO has been reported to occur in approximately 63%-65% of service members with limb loss or major extremity injuries during Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF). Reports of recent OIF/OEF combat-related amputees with known HO have indicated that approximately 20-40% of affected patients required surgery to excise bony masses. HO may cause skin ulcerations, chronic pain, and delay rehabilitation regimens, as ectopic bone resection often requires modifications to the prosthetic limb.
Determining the appropriate time for HO removal remains a challenge given the likelihood of multiple trauma and neurological conditions that accompany the bone injury. While results from early ectopic bone resection have remained promising, premature removal may result in florid regrowth requiring a secondary surgical procedure. Therefore, Dr Isaacson and his Team are investigating if advanced histological techniques may be a better predictor of HO growth/development so that patient-specific surgical schedules may be used to reduce recurrent bone growth.
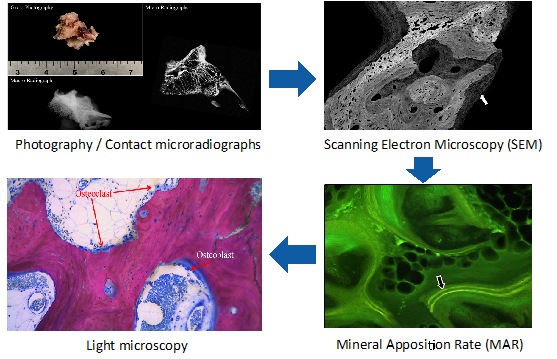
Preliminary data from the Bone & Joint Research Laboratory has indicated that the mineral apposition rate (MAR) of resected HO specimens were approximately 1.6 times higher than non-pathological human bone. Elevated MAR levels were supported by scanning electron microscopy (SEM) images, which demonstrated HO to be a highly vascular network in varying stages of regrowth. Despite clinical predictors of HO maturity, histological data indicated that the ectopic bone resected from wounded warfighters were still immature even at the time of surgical intervention (average 10.5 +/- 7.1 months from the date of injury). That is, the ectopic bone had not completed its growth pattern.
Data analysis from the first fifteen (15) service members enrolled in this study have demonstrated that pre-operative alkaline phosphatase (AP) levels were an effective measuring tool for assessing the extent of HO growth in situ. Alkaline phosphatase (AP) is a enzyme found in all body tissues, to include bone. Pre-operative AP levels were highest for those with below the knee amputations, followed by above the knee and upper extremity injury. However, before conclusions can be made on AP levels and injury location, further data analysis will be required to screen for accompanying orthopedic injuries since the occurrence of accompanying fractures would likely increase AP levels.
Lastly, when the non-steroidal anti-inflammatory drug (NSAID) was assessed as a variable in the study, the number of single tetracycline labels strongly correlated with HO recurrence. This finding supported the use of tetracycline labeled bone biopsies as a tool for assessing HO stages for removal in the future. Taken together, these analyses may improve care for wounded warriors afflicted with HO, potentially permitting earlier excision in some symptomatic patients and avoiding post-excision HO recurrence in others.
References:
[1] Isaacson BM, Stinstra JG, MacLeod RS, Pasquina PF, Bloebaum RD. Developing a quantitative measurement system for assessing heterotopic ossification and monitoring the bioelectric metrics from electrically induced osseointegration in the residual limb of service members. Annals of Biomedical Engineering. 2010;38:2968-78.
[2] Isaacson BM, Brown AA, Brunker LB, Higgins TF, Bloebaum RD. Clarifying the structure and bone mineral content of heterotopic ossification. The Journal of Surgical Research. 2011;167:e163-70.
[3] Isaacson BM, Weeks SR, Pasquina PF, Webster JB, Beck JP, Bloebaum RD. The road to recovery and rehabilitation for injured service members with limb loss: a focus on Iraq and Afghanistan. US Army Medical Department Journal 2010:31-6.
[4] Forsberg JA, Pepek JM, Wagner S, Wilson K, Flint J, Andersen RC, et al. Heterotopic ossification in high-energy wartime extremity injuries: prevalence and risk factors. J Bone Joint Surg Am. 2009;91:1084-91.
[5] Forsberg JA, Potter BK. Heterotopic ossification in wartime wounds. J Surg Orthop Adv. 2010;19:54-61.
[6] Potter BK, Burns TC, Lacap AP, Granville RR, Gajewski DA. Heterotopic ossification following traumatic and combat-related amputations. Prevalence, risk factors, and preliminary results of excision. The Journal of Bone and Joint Surgery American Volume. 2007;89:476-86.
[7] Isaacson BM, Swanson TR, Potter BK, Pasquina PF. Tourniquet use in combat injured service members: a link with heterotopic ossification? (Accepted to Journal of Orthopedic Research & Reviews).
[8] Bloebaum RD, Bachus KN, Momberger NG, Hofmann AA. Mineral apposition rates of human cancellous bone at the interface of porous coated implants. Journal of Biomedical Materials Research 1994;28:537-44.
Acknowledgements: This material is based upon work supported by the Department of the US Army under Award Numbers W81XWH-12-2-0017 to the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (Fort Detrick, MD) and the Center for Rehabilitation Science Research USU Award NF90UG, (Bethesda, MD).