



- Phase II Study of Her2 Intracellular Domain Peptide-Based Vaccine Administered to Locally Advanced and Metastatic Her2+ Breast Cancer Patients Receiving Trastuzumab
- The Role of Progesterone and Estrogen in Breast Cancer Risk - Implications on Breast Cancer Therapy
- Breast Cancer Suppression by IDO Inhibitors
- Using SPECT-CT Imaging to Reduce Radiation Therapy-Induced Lymphedema in Breast Cancer Patients
Phase II Study of Her2 Intracellular Domain Peptide-Based Vaccine Administered to Locally Advanced and Metastatic Her2+ Breast Cancer Patients Receiving Trastuzumab
Posted October 4, 2011
Mary (Nora) L. Disis, M.D., University of Washington
Clinical Translational Research Award
In this year alone, approximately 230,480 women in the United States will be diagnosed with invasive breast cancer, and up to 30% of those women will have recurrence within 5 years of primary therapy. Dr. Nora Disis, a recipient of a Fiscal Year 2003 Breast Cancer Research Program Clinical Translational Research Award, developed a vaccine that, when concurrently administered with trastuzumab (Herceptin), strongly elicits an immune response to the growth factor receptor HER2, generating long-term tumor-specific immunity. The HER2 intercellular domain (ICD) peptide-based vaccine is designed to treat breast cancer by stimulating the immune destruction of remaining cancer cells after primary cancer therapy. The HER2 ICD peptide vaccine is being evaluated in a Phase II Clinical Trial that recruited 38 stage III and stage IV HER2+ breast cancer patients concurrently receiving trastuzumab. While data acquisition is not yet complete, interim analysis on the first 25 patients suggests considerable improvements in relapse-free survival in the vaccinated patients without significant side effects. The historical relapse-free survival at 4 years for the enrolled patient cohort is 44%. Interim analysis on the first 25 vaccinated patients indicated improved progression-free survival: relapse-free survival after 1 year after vaccination is estimated to be 82%; after 2 years, it is estimated to be 63%. Importantly, neither significant cardiac toxicity nor autoimmune responses have been reported thus far. Preliminary data suggest that the vaccinated patients develop significant augmentation of immunity to HER2 and that most patients developed immunity against other tumor antigens (epitope spreading), which is associated with improved survival. Overall survival analysis of the first 25 patients is scheduled to be completed in November 2011.
Publication:
Disis ML, Wallace DR, Gooley TA, Dang Y, Slota M, et al. 2009. Concurrent trastuzumab and HER2/neu-specific vaccination in patients with metastatic breast cancer. Journal of Clinical Oncology 27(28):4685-4692.
Links:
The Role of Progesterone and Estrogen in Breast Cancer Risk - Implications on Breast Cancer Therapy
Posted June 28, 2011
Sandra Z. Haslam, Ph.D., Michigan State University, East Lansing, Michigan
FY06 Breast Cancer Research Program Idea Award, BC061158
Hormone replacement therapy (HRT) was a common treatment option for alleviating menopausal symptoms, until a large clinical trial in 2002 found a link between HRT and several health hazards, including increased risk of breast cancer. While both estrogen and progesterone are implicated in the etiology of breast cancer, women receiving both estrogen and progesterone during HRT developed more aggressive cancers when compared to women receiving only estrogen. Although the role of estrogen in breast cancer has been widely studied, the underlying mechanisms of progesterone-mediated oncogenesis are largely unknown.
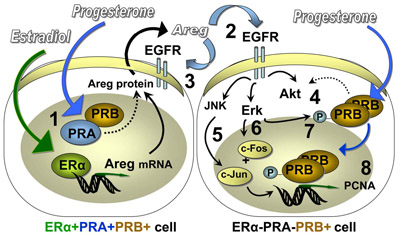
Supported by a Fiscal Year 2006 Breast Cancer Research Program Idea Award, Dr. Sandra Haslam has established how progesterone and estrogen interact to promote both normal and cancer cell growth in the breast. Her studies have provided clues for how these hormones contribute to breast cancer development, which may lead to novel treatment strategies for hormone-dependent subtypes of breast cancer. During her studies, Dr. Haslam found that exposure to both estrogen and progesterone was more potent than estrogen alone in promoting cellular proliferation in both normal mammary glands and in tumors in rats. She demonstrated that estrogen and progesterone work together to induce the production of amphiregulin (Areg), an epidermal growth factor receptor (EGFR) ligand, inducing robust cellular growth. Moreover, Areg interacts with progesterone via progesterone receptor B, promoting further tumor growth. Since this research was carried out using the natural endogenous hormone, progesterone, this indicates that progesterone that is used in bioidentical formulations of hormonal therapies pose the same risks for breast cancer development as the synthetic hormones used in conventional menopausal hormone therapies.
Dr. Haslam's findings suggest that simultaneous inhibition of estrogen and/or progesterone in addition to EGFR may be an effective treatment strategy for women with hormone-dependent breast cancer, which may be especially important in premenopausal women who produce both estrogen and progesterone.
A diagram of convergence of E, P, an EGFR signaling pathways in the normal rat mammary epithelial cells.
Publication:
Kariagina A, Xie J, Leipprandt JR, and Haslam SZ. 2010. Amphiregulin mediates estrogen, progesterone, and EGFR signaling in the normal rat mammary gland and in hormone-dependent rat mammary cancers. Horm Cancer 1(5): 229-244.
Links:
Breast Cancer Suppression by IDO Inhibitors
Posted March 22, 2011
George C. Prendergast, Ph.D., Lankenau Institute for Medical Research, Wynnewood, Pennsylvania
Indoleamine 2,3-dioxygenase (IDO) is an enzyme which regulates the levels of tryptophan, an amino acid that is essential for T cell function. Elevation of IDO depletes the level of tryptophan in local tissue environments, blocking the activation of T cells. IDO is commonly overexpressed in breast cancer, and is implicated in preventing an anti-tumor immune response, enabling tumor cells to survive, and contributing to the progressive loss of immunosurveillance and tumor cell destruction as the disease advances. With support from the Department of Defense Breast Cancer Research Program (BCRP), Dr. George Prendergast established IDO as a target for cancer treatment and identified several novel inhibitors of IDO, some of which are currently in clinical trials for recurrent or refractory solid tumors, including breast cancer.
In Fiscal Year 2002, Dr. Prendergast was awarded a Breast Cancer Research Program Idea Award to identify lead inhibitors of IDO that have better potency than an existing inhibitor, 1-methyl-DL-tryptophan (1MT). At the time of the award, IDO had not been confirmed as a target for breast cancer therapy. Dr. Prendergast hypothesized that inhibiting IDO in breast cancer will promote an immune response against the tumor. He identified several novel IDO inhibitors, some of which exhibited significantly greater potency than 1MT. Moreover, Dr. Prendergast demonstrated that IDO inhibitors work synergistically with existing chemotherapeutic agents (e.g., taxanes) without increased side effects in mouse models of breast cancer.
At the time of the award, IDO was thought to be unique and not a part of a larger gene family. When Dr. Prendergast observed that the D isomer of 1MT (D-1MT) had more active antitumor activities than the L isomer without actually inhibiting the IDO enzyme, he looked for IDO-related genes and discovered IDO2/INDOL1, later established to be D-1MT's actual target. D-1MT has since entered Phase I clinical trials for breast cancer and other cancers, alone or in combination with other drugs. Dr. Prendergast notes, "the unusually rapid translation of IDO inhibitors from an obscure stage of preclinical study to Phase I clinical trials seeded by this DoD project represents an unusual and notable success for the DoD Breast Cancer Research Program."
Publications:
Muller AJ, DuHadaway JB, Donover PS, Sutanto-Ward E, and Prendergast GC. Inhibition of indoleamine 2,3-dioxygenase, a target of the cancer suppression gene Bin1, potentiates cancer chemotherapy. Nature Med 2005 Mar; 11(3): 312-9.
Muller AJ, Malachowski WB, and Prendergast GC. IDO in cancer: targeting pathological immune tolerance with small molecule inhibitors. Expert Opin Ther Targets 2005 Aug; 9(4): 831-49.
Muller AJ and Prendergast GC. Indoleamine 2,3-dioxygenase in immune suppression and cancer. Curr Cancer Drug Targets 2007 Feb;7(1): 31-40.
Links:
Public and Technical Abstracts: Breast Cancer Suppression by IDO Inhibitors
Using SPECT-CT Imaging to Reduce Radiation Therapy-Induced Lymphedema in Breast Cancer Patients
Posted January 27, 2011
Andrea L. Cheville, M.D., Mayo Clinic and Foundation, Rochester, MinnesotaRadiotherapy is one of the primary treatment options available to breast cancer patients. Radiation often causes irreversible damage to the axillary lymph nodes, resulting in lymphedema, a chronic swelling of tissue in the arms caused by the retention of lymphatic fluid. In addition to pain and discomfort in the affected limb, patients with lymphedema are more likely to develop limb impairments, such as restricted range of motion, as well as recurring infections. Lymphedema, which can develop over several years, may affect up to as many as 70% of women that undergo radiotherapy, yet there is no cure. Current treatment strategies are limited to compression, massage, bandage wrapping, and exercise.
Dr. Andrea Cheville, recipient of a Fiscal Year 2002 Breast Cancer Research Program Physician-Scientist Training Award, has utilized a novel imaging technique that integrates single photon emission computed tomography (SPECT) with computerized tomography (CT) scans (SPECT-CT). This innovative method is capable of precisely locating those lymph nodes which are critical for fluid drainage from the arms, allowing physicians to minimize unnecessary exposure. Using SPECT-CT, Dr. Cheville assessed changes in lymph drainage patterns after radiation therapy in patients without lymph node metastases and determined the critical lymphatic structures associated with lymphedema. The results indicated that only a few lymph nodes (among up to 62 under the armpit) are involved in fluid drainage, and that almost half of the patients received potentially damaging doses of incidental, non-beneficial radiation to these structures. In light of these results, Dr. Cheville is monitoring the development of lymphedema in patients who received standard radiation treatment against patients who received a modified treatment demonstrated to reduce incidental radiation by utilizing SPECT-CT. Protecting the critical lymph nodes is expected to dramatically reduce the occurrence of lymphedema - no cases of lymphedema have yet been reported - improving patients' long-term quality of life after radiotherapy for primary breast cancer.
Links: