



Lung Cancer



Posted October 30, 2020
E. Premkumar Reddy, Ph.D., Icahn School of Medicine at Mount Sinai

Non-small cell lung cancer (NSCLC) is a common form of lung cancer, exhibiting the mutation of the oncogene, KRAS, in approximately 15-20% of cases. KRAS is important for producing the KRAS protein, which plays a central role in transmitting signals for cell growth, division, and destruction (apoptosis) through the RAS/mitogen-activated protein kinase (RAS/MAPK) pathway. When activated, the K-RAS protein can relay signals from outside a cell to the cell’s nucleus, delineating cell fate. When mutated to a constitutively active form, the KRAS gene can cause normal cells to become cancerous. Naturally, many researchers have focused their attention on targeting RAS-driven signaling to treat NSCLCs; however, the lack of available binding sites for potential inhibitors on the surface of the RAS protein has impeded the progress in this area.
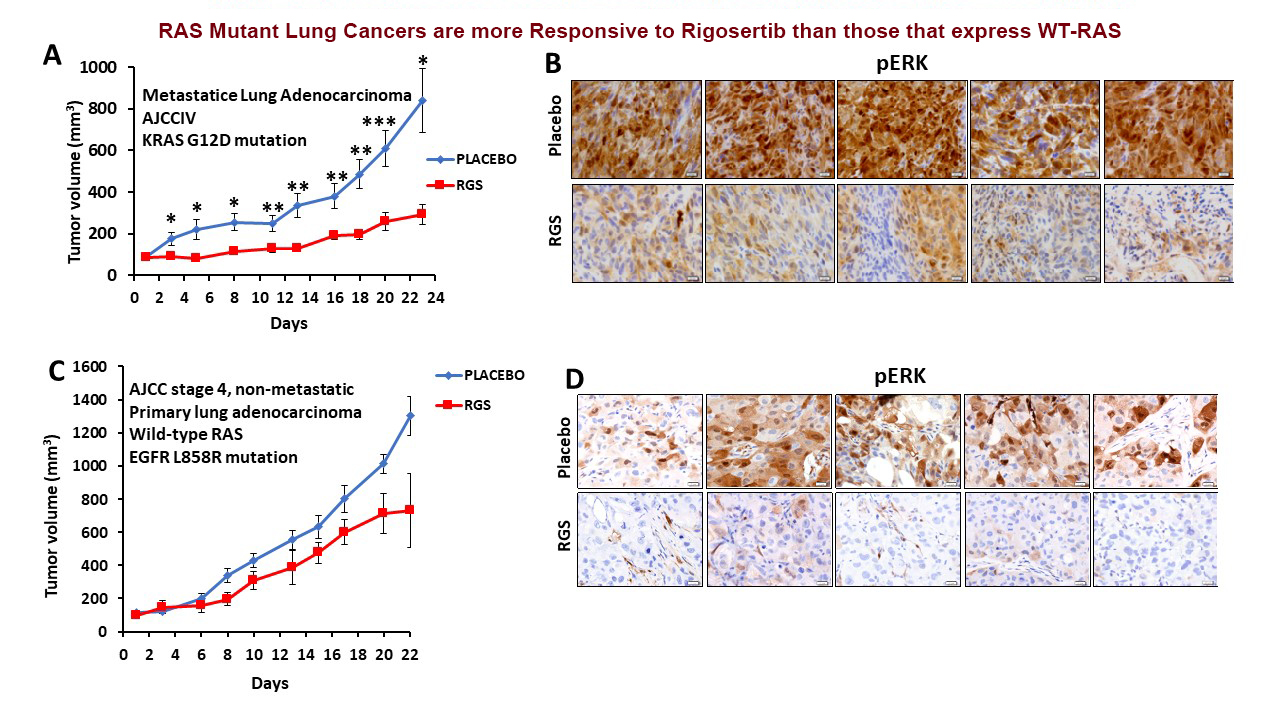
With funding from a Fiscal Year 2016 (FY16) Lung Cancer Research Program (LCRP) Investigator-Initiated Translational Research Award, Dr. E. Premkumar Reddy at the Icahn School of Medicine at Mount Sinai sought a solution to the RAS-binding challenge by employing a unique strategy: creating inhibitors that would bind to specific areas of RAS effectors and prevent their interaction with RAS (RAS mimetics), thereby turning off unwanted cell signaling. To accomplish this task, Dr. Reddy and his team screened a novel chemical library and identified rigosertib (RGS), a small molecule that binds to the conserved RAS Binding Domain (RBD) of RAS effectors. Dr. Reddy’s laboratory also developed a new compound, 015040, which displayed a marked affinity in RBD binding, inhibited RAS-driven signaling, suppressed the growth and induced apoptosis of NSCLC cell lines. Armed with a new strategy to inhibit RAS-activated signaling pathways, Dr. Reddy and his team hypothesized that RGS and 015040 would inhibit KRAS-mutant lung tumor growth.
Using both genetically engineered mouse models and patient-derived xenograft (PDX) models of lung cancer, Dr. Reddy sought to determine the therapeutic effects of RAS mimetics in this disease. Preliminary studies of two primary PDX metastatic lung adenocarcinoma tumor models were promising; however, results were disappointing when genetically modified mouse models of mutant KRAS-driven lung tumors were treated with RGS administered through intraperitoneal (ip) injection, as tumor growth did not regress. They noted that the dosage and method of administration of RGS greatly influenced bioactivity of the compound. In fact, when RGS levels in plasma samples were examined using liquid chromatography and mass spectrometry, data suggested that oral delivery of RGS at a dose that is the equivalent of that which was established in Phase I clinical trials, as opposed to ip injection, was more efficient at achieving levels of RGS in the plasma that are of therapeutic concentration. A small cohort of mutant KRAS mice was therefore treated via ingestion of a custom RGS chow. Histological and immunohistochemical staining of lungs from these mice confirmed the therapeutic benefits of the diet as noted by reduced tumor growth. Currently, Dr. Reddy and his team are expanding this efficacy study in a larger cohort of animals.
Researchers in Dr. Reddy’s laboratory also explored the therapeutic effects of a combination of RAS mimetics with anti -programmed death-ligand 1 (PDL1) immune checkpoint therapy. Using the same mutant KRAS mouse model, they found that treatment with anti-PDL1 antibodies did not have a significant therapeutic effect on tumor growth in mice treated with anti-PDL1 antibodies in combination with RGS (given by ip injection). Because of the previous results describing improved administration of RGS via diet, the team has repeated this combination study with using oral route of administration. Preliminary studies suggest that combination of RGS with anti-PDL1 is effective at reducing the lung tumor burden in the genetically modified mutant KRAS mouse model.
Additionally, Dr. Reddy sought to elucidate possible mechanisms through which lung tumor cells may acquire resistance to RGS by isolating RGS-resistant clones and screening them using the Cancer Tool Kit (CTK) developed by collaborator, Dr. Kris Wood, from Duke University. The CTK screening includes a library of genes across 17 cell signaling pathways often implicated in tumor progression. Resistance studies in the mutant KRAS-dependent NSCLC cell line, H358, suggested that mutations in the JAK-STAT and MEK pathways (which affect cell survival, growth, and differentiation) cause resistance to RGS in vitro. Currently, Dr. Reddy’s team is in the process of extending these results to other NSCLC cell lines, further examining the role these mutations may play in lung cancer and exploring observed long-term effects of RGS treatment in NSCLC, such as cell senescence.
Importantly, based on these studies funded by the LCRP, a Phase I/IIa clinical trial has been initiated with collaborators from Mount Sinai, Bristol-Myers Squibb and Onconova Therapeutics, Inc. The trial, “A Phase1/2a Study of Rigosertib Plus Nivolumab in Stage IV Lung Adenocarcinoma Patients with KRAS Mutation Who Progressed on First-Line Treatment,” headed by Dr. Rajwanth Veluswamy of Icahn School of Medicine at Mount Sinai will focus on RAS-mutant lung cancer patients in order to study the therapeutic effects of RGS in combination with checkpoint inhibitors. Dr. Reddy and his collaborators hope that results from this promising new RAS-mimetics technique will lead to new life-saving therapeutic approaches for patients experiencing KRAS NSCLC.
Link:
Clinical trial (NCT04263090; https://clinicaltrials.gov/ct2/show/NCT04263090).
Last updated Thursday, May 26, 2022